|
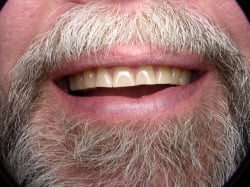
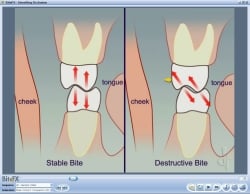
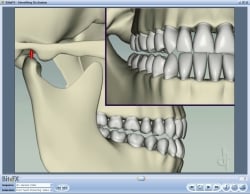
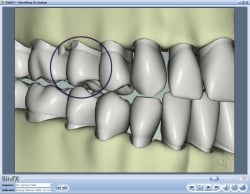
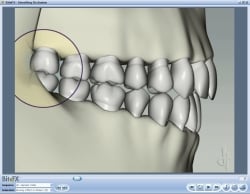
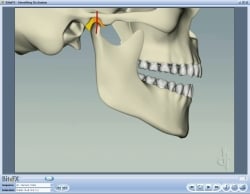
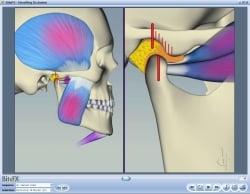
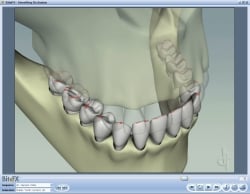
This is an article written by Dr. Reid and published a few years back in Dentistry Today. It is still relevant today - though we'd probably say "maximum intercuspation" (MIP) rather than "centric occlusion" (CO). You can read it in its original form as a PDF "Presenting Occlusal Disease in 3-D for Greater Case Acceptance" or as reproduced below for this blog. Occlusal disease is one the most destructive and neglected elements in dentistry, and plays a major role in reducing the longevity of our finest restorative efforts. It can present itself in the form of painful, clicking TM Joints, sore facial muscles, headaches, tooth wear, tooth looseness, sensitivity, and migration. It is a dominant factor in the fracture of restorations on posterior teeth. Although a dentist may understand the cause and effect of these destructive forces, explaining these concepts to patients and their families can be very difficult. It is much easier to discuss the solution for caries or fractured teeth than it is to describe how excess wear is caused by a movement of the mandible from maximum intercuspation, in and out of centric relation position. Likewise understanding how interferences on the balancing or non- working side during lateral excursions is difficult enough for dentists to see and detect, this difficulty is only compounded when we try to explain these problems to patients. Difficult or not, we are obligated to offer a treatment plan for the resolution of all disease categories which fall within our scope of health care service. Case ReportA middle aged male came into my practice wanting to replace a missing lower tooth No. 24 due to trauma and restore broken molar No. 31 (Figure 1). His only request was that we not use gold on the molar as he had in the past, but rather some of the newer porcelain crowns he’d seen and heard about through the media that would match his existing coloration. A pre-clinical interview was conducted during which we discussed specific long term goals and objectives. Full mouth radiographs, 9 intraoral photographs (Canon Digital Rebel), panorex and mounted study models (SAM 3 Articulator [Great Lakes Orthodontics]) in centric relation were taken. A complete examination was conducted evaluating the TMJ, muscles, periodontal structures, cancer evaluation, and occlusion. The tooth-by-tooth exam looking for excess wear, looseness, fractures and caries was aided by the use of a dental operating microscope (Global Protégé). Initial findingsThe patient’s goal was to keep his natural teeth for a lifetime (Figure 1) and he expressed a desire for his dental team to help him achieve a more healthy and comfortable mouth. The health history was unremarkable. The patient was aware of grinding his teeth during sleep as he would wake on occasion to facial pain. The periodontal examination revealed a healthy mouth with a mild localized gingivitis. The missing lower front tooth was recently removed and successfully grafted. There was mesial drifting of No. 23. Caries was incipient (DIAGOdent [KaVo]) and confined to occlusal surfaces only. This patient had a very healthy mouth as it relates to the teeth and periodontal tissues. However, the signs of occlusal disease were everywhere and significant in nature. This was evidenced by the following findings: muscles were palpated and on a scale from 1-10 with 10 being exceptionally tender, displayed a 6 on the belly of the masseters bilaterally. The anterior fibers of the temporalis were an 8 on the left and 5 on the right. Both medial ptyergoids were very painful upon minimal palpation. The TMJ had no pain upon palpation and had an early opening and late closing click upon full opening to 50 mm. There was no deviation on opening and normal ability to move the jaw side-to-side 10 to 15 mm. The Doppler auscultation (Great Lakes Orthodontics) examination was normal on rotation and revealed slight crepitus sounds upon translation. Centric relation position was determined using bimanual manipulation, and the first tooth in contact was in fact, the broken and loose molar No. 31. From CR there was a 2 mm forward slide into CO. The, large wear facet on No. 31 had its distal origin in CR when evaluated with thin articulating paper. Occlusal exam showed minimal yet sufficient separation of the posterior teeth in protrusive motion. There was group function with balancing interferences during lateral movements bilaterally. (Figure 2). Not surprisingly, given the findings above, the buccal cusp tips of all maxillary posterior teeth displayed wear facets into dentin (Figure 3). The maxillary first and second premolars had class 2 mobility, and there was pronounced recession on the facial surface of the first premolars. This patient was doing more harm to his teeth due to the destructive forces of an unstable bite than from disease caused by bacterial origin. My intent was to help him appreciate the severity of his occlusal disease and see the need for a comprehensive treatment plan to address his needs. The patient was invited back for a treatment consultation. Seeing the ProblemI began my consultation by discussing my role in establishing ideal tooth contact (BiteFX software, Figure 4). Given his desire for a porcelain restoration instead of a gold one, the patient quickly grasped the importance of addressing his occlusal problems when shown a digital photo of the ideal vs. actual contacts on his own teeth (Figures 3 and 5). I explained that this type of severe and improper contact would wear through gold but could fracture glass! Role of Front TeethI then relayed an analogy of fence posts withstanding vertical forces but not doing well if repeatedly backed into by a pickup truck, so that the patient readily understood the idea of the back teeth hitting in ideal contact and the forces being directed vertically to accomplish stable occlusion. I watched the eyebrows rise as I showed him ideal canine guidance during lateral jaw movement using animations. (Figure 6). The animation used to demonstrate how lack of canine guidance can harm rear teeth was extremely helpful for his treatment decisions (Figure 7). I then directed him to a previous picture (Figure 3) and observed as he acknowledged the magnitude of his newly discovered problem. When shown animations of tooth looseness caused by destructive forces (Figure 8), issues of mobility and wear were understood simultaneously. The Remaining and Critical ConceptCentric relation position of the TMJ during biting is the border position that allows the restorative dentist to ‘perfect and protect ‘the bite from destructive forces. Using BiteFX animations (Figures 9 and 10) the patient understood the source of his wear and the meaning of the initial tooth contact on No. 31 (the slide). The beauty of distributing the force over the largest area possible to minimize stress (stress = force/area) was highlighted by reinforcing proper tooth contact as all teeth hit simultaneously (Figure 11). A Win-Win NoPressure Treatment PlanThe treatment plan that met the original chief complaint included minimally invasive operative dentistry, a porcelain crown on the broken molar, placing an implant and implant-supported crown in site No. 24, and a full-coverage maxillary bruxism appliance (permissive type). He was informed the appliance would be mandatory during sleep and all other times when he was aware of clenching or grinding, i.e. working in his shop, while driving etc. I explained this would be a lifelong requirement. I then presented an alternative treatment option more consistent with his personal goals for natural looking teeth combined with his desire to avoid the commitment to wearing an appliance. I explained that he could achieve built-in protection with a minimally invasive approach to include occlusal equilibration and all ceramic veneers to restore anterior guidance. Together we viewed photos of his smile and decided a minimal of eight maxillary restorations would be acceptable aesthetically. At this point the patient made a decision to alter the color of his smile whereas he originally wanted to have a crown to match his existing coloration. He understood that he may have additional elective veneers in the future and would still maintain the desired function to contain the destructive forces of his occlusal disease. The mutually understood treatment plan was thoroughly outlined, the cost discussed, and the patient readily accepted it. The treatment plan included the following:
Getting StartedAfter achieving optimum oral health with the hygienist, an occlusal equilibration was performed simultaneously with an intraoral mock-up of the maxillary 8 teeth (Figures 12 and 13). The goal of having centric occlusion in harmony with centric relation combined with anterior guidance was attained. More importantly, the patient could take this new smile for a “test drive” evaluating for comfort, function, speech, interferences and the look of the transformed bite. After several months the new teeth did not show any evidence of wear, no noxious habits had been developed and the patient did not report any discomfort. The maxillary premolars became nonmobile. Final PreparationsMy examination confirmed that the mandible moved loosely and freely into centric relation and all teeth contacted ideally, i.e. simultaneously upon guided or unguided closure. The teeth shape and position had been pre-approved and test driven. Now the fun began. Prior to preparation, impressions of the teeth were taken as a matrix for the provisional restorations. The teeth were minimally prepared (Figures 14 and 15 ) using Brassler diamonds. Centric relation bite records were taken using Futar D (Roydent) as well as a facebow transfer to a SAM 3 semiadjustable articulator. Final full-arch impressions were taken of both arches using vinyl polysiloxane (Splash! [Discus Dental]). This technique combined with use of the Axio-quick bite fork (SAM 3), eliminates the need for the dentist to either mount or pour the models. Stump shades as well as final restoration shades were determined as the final restorations would be refractory feldspathic porcelain veneers. The provisional restorations were fabricated chairside (Figures 16 and 17) using Luxatemp Floresence (Zenith/DMG) and bonded in place using Luxaflow (Zenith/DMG). Models of the completed temporaries were taken using Alginot (Kerr Dental) to eliminate the need to pour models. A centric relation bite record of the temporaries using Futar D was recorded. Digital photos of the provisional were provided for the lab. The final restorations were placed using RelyX (3M ESPE) translucent veneer cement. (Figures 18 and 19). ConclusionThis case is presented as one in progress. The lower implant placement was performed and, between writing this article and its publication, the patient elected to restore the lower anterior with porcelain restorations to compliment his upper teeth (Figure 20). Additionally, he has expressed a desire to “add” one more restoration to enhance the appearance of his biggest smile. My original intent was to help my patient achieve optimum oral health, comfort and function and to offer solutions to the obvious destruction occlusal disease had caused. His desire to have a more pleasing smile was solved in a conservative fashion, and provided the solution to excess wear, as well as tooth mobility and fracturing. The occlusal philosophy of functionally created anterior guidance in harmony with centric relation and centric occlusion, allows the dentist to offer the very minimal dentistry needed to achieve desired health goals. Once stabilized, the patient has the luxury of proceeding with future care when it suits his personal desires and financial abilities. This treatment plan was developed with the desires of the patient in mind. The visual presentation given to the patient, permitted him to understand the detrimental effects of occlusal disease and allowed him to “see for himself” the harmful effects of his current condition. When the advantages of treating this problem were understood using the power of visual learning (BiteFX), the patient immediately realized that his personal goals of improving his appearance and achieving healthy dentition were within his grasp. |
|
 Donald Reid, DDS
Donald Reid, DDS